Not for the Lazy, this takes a lot of work!
The treatment prescribed for you, or your child’s amblyopia will depend on various factors.
- What type of amblyopia.
- Age of the patient.
- Compliance.
Treatments include eye patches, drops, glasses or contact lenses, virtual reality headset, and sometimes surgery.
Corrective eyewear. Glasses or contact lenses can correct problems such as nearsightedness, farsightedness, or astigmatism that result in lazy eye.
Eye patches or occlusion therapy involves blocking the vision in one eye (generally the “good” eye) allowing the other eye to do all the work. (I told you this wasn’t for the lazy).
To stimulate the weaker eye, your child wears an eye patch over the eye with better vision for two to six or more hours a day. In rare cases, wearing an eye patch too long can cause amblyopia to develop in the patched eye. However, it’s usually reversible.
Eye patches are available as adhesive patches that adhere to the area around the eye, preventing any light or vison in the covered eye. These may cause irritation to the sensitive skin around the eye, but there are tricks to help with this. The majority of pediatric ophthalmologists will prescribe occlusion therapy with adhesive patches to ensure compliance.
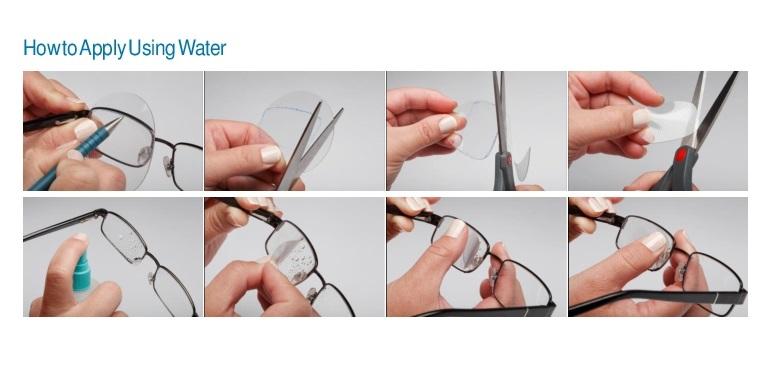
If a child wears glasses, a cloth eye patch may be an option. This type of patch attaches to the glasses to occlude the vision. The drawback is the child has the opportunity to peek around or over the patch. There is no skin irritation. They may be reused.
A pirate patch is a patch that has a strap that holds the patch over the eye. The occlusion portion may be cloth, plastic, or silicone. This is an option if glasses are not won. This method is easy to peek around.
Eyedrops. An eyedrop of a medication called atropine (Isopto Atropine) can temporarily blur vision and is applied in the stronger eye. Usually prescribed for use on weekends or daily, use of the drops encourages your child to use the weaker eye and offers an alternative to a patch. Side effects include sensitivity to light and eye irritation.
Surgery. Your child might need surgery if he or she has droopy eyelids or cataracts that cause deprivation amblyopia. If your child’s eyes continue to cross or wander apart with the appropriate glasses, your doctor might recommend surgical repair to straighten the eyes, in addition to other lazy eye treatments.
Activity-based treatments — treatments offered may be drawing, doing puzzles, virtual reality headsets, or playing computer games. The effectiveness of adding these activities to other therapies may vary and has not been proved. However, research into new and non-traditional treatments is ongoing.
For most children with lazy eye, proper treatment improves vision within weeks to months. Treatment might last from six months to two years.
Remember, it is important for your child to be monitored for recurrence of lazy eye — which can happen in up to 25 percent of children with the condition. If lazy eye recurs, treatment will need to start again.
Lazy eye (amblyopia) – Diagnosis & treatment – Mayo Clinic
Occlusion Therapy – Eye Patches – Fresnel Prism and Lens (fresnel-prism.com)